
TL;DR:
- Hospitals are essential for integrating genetic testing, interpretation, and patient counseling into comprehensive genomic screening programs. They face technical, staffing, and infrastructure challenges but can succeed by prioritizing workflow design, EHR integration, and patient engagement practices. Implementing AI tools and strong data governance enables hospitals to deliver more effective, accessible, and sustainable genomic care.
Hospitals are the primary delivery point for genomic screening services, responsible for integrating genetic testing, clinical interpretation, and patient counseling into a single coordinated care model. A Mayo Clinic study found that approximately 1 in 8 adults carries a hidden genetic risk for a significant health condition. That figure defines the scale of what hospitals must address. The role of hospitals in genomic screening goes far beyond ordering a lab test. It requires multidisciplinary teams, interoperable digital infrastructure, and a patient engagement model built around trust and informed consent. Tools like next-generation sequencing (NGS) and AI-driven platforms such as GeneMatrixAI are reshaping how hospitals deliver this work at scale.
What are the core clinical workflows in hospital genomic screening?
Hospital genomic screening programs follow a structured clinical pathway. Each step depends on the one before it, and a failure at any stage reduces the program's clinical value.
- Pre-test counseling. Genetic counselors review the patient's personal and family history, explain what the test can and cannot reveal, and obtain informed consent. This phase sets expectations and prepares patients for results that may carry significant psychological weight.
- Sample collection. Hospitals collect blood or saliva samples depending on the test panel ordered. Both methods are clinically validated for most hereditary cancer and pharmacogenomic panels.
- Laboratory sequencing. Samples move to a CLIA-certified lab where NGS platforms generate raw genetic data. Quality controls at this stage filter out low-confidence reads before analysis begins.
- Data interpretation. A medical geneticist or trained genomics specialist reviews variant calls against curated databases such as ClinVar and OMIM. This is where the complexity concentrates.
- Results communication. Genetic counselors translate findings into clinical language, coordinate with the treating physician, and schedule a post-test session with the patient.
- EHR integration. Genomic results are entered into the patient's electronic health record as structured, searchable data rather than static PDF attachments.
The multidisciplinary team typically includes genetic counselors, medical geneticists, laboratory scientists, oncologists, and primary care physicians. Each role is defined, and overlap is intentional. Genomics-based patient management works best when these specialists communicate through shared clinical records rather than siloed reports.
Pro Tip: Map your hospital's current genomic workflow against this six-step model before purchasing new technology. Most implementation failures trace back to gaps in steps 1 or 6, not the sequencing itself.

How do hospitals overcome technical and staffing challenges?
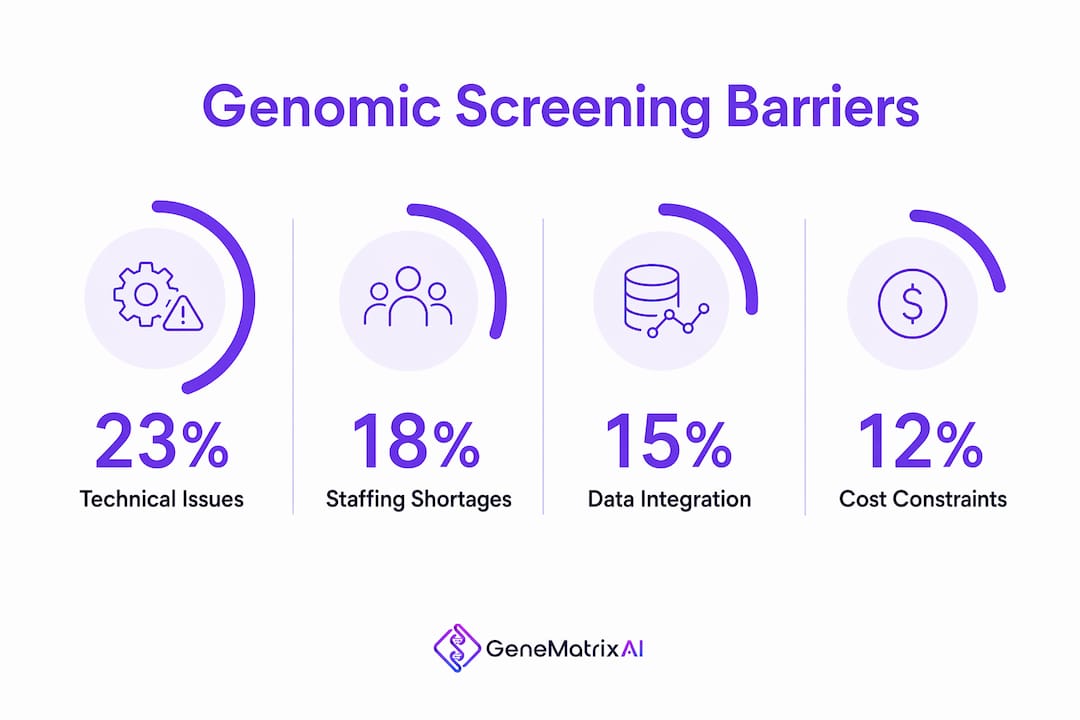
The barriers to scaling genomic medicine in hospitals are well documented. Technical barriers break down as follows: 23% relate to NGS technology limitations and 15% stem from complexity in data interpretation pipelines. Those two categories alone account for more than a third of all implementation friction.
The staffing problem compounds the technical one. The real bottleneck in hospital genomic programs is downstream clinical interpretation by genetic counselors, not the sequencing hardware. As testing volume grows, counselor capacity becomes the limiting factor. Most hospital systems have not scaled their genetics workforce to match the demand created by expanded screening panels.
Hospitals that have successfully addressed these challenges share several operational strategies:
- AI-assisted interpretation. AI-driven platforms help overcome workforce shortages by automating variant classification and flagging clinically significant findings for human review. This does not replace genetic counselors. It allows them to focus on complex cases.
- Lab partnerships. Hospitals that partner with genomic laboratories reduce capital expenditure on sequencing equipment while maintaining clinical control over interpretation and patient communication.
- Health Institution status. Hospitals operating under Health Institution status for in-house genomic testing avoid the prolonged regulatory performance studies required for commercial kits. This creates meaningful operational agility.
- Interoperable IT infrastructure. Investing in platforms that connect genomic data to existing EHR systems prevents the data silos that make genomic results clinically useless after the initial report.
- Workforce development. Structured training programs for nurses, primary care physicians, and pharmacists extend the reach of a small genetics team without requiring new hires at every level.
AI in healthcare diagnostics is not a future consideration for hospital genomic programs. It is a present operational requirement for any system running more than a few hundred tests per month.
Pro Tip: Before investing in an AI genomics platform, confirm it integrates directly with your EHR vendor. A platform that produces a separate report rather than writing structured data into the patient record adds work instead of removing it.
Why does EHR integration define the value of genomic data?
Genomic data locked in a PDF has no clinical value after the day it is printed. Successful hospital programs embed genomic results directly into clinical records as actionable, searchable data that informs every future care encounter. That distinction separates programs that improve outcomes from those that generate reports.
The table below compares static genomic reporting against integrated genomic records across four clinical dimensions.
| Dimension | Static PDF Report | Integrated EHR Record |
|---|---|---|
| Accessibility | Single-use, manually retrieved | Searchable across care settings |
| Clinical decision support | None at point of care | Triggers alerts and care pathways |
| Longitudinal use | Rarely revisited | Updated and referenced over time |
| Preventive care impact | Limited to initial encounter | Informs ongoing risk management |
Hospital leaders must move beyond single-organization data silos to interoperable systems that allow genomic data to move with the patient across departments and care settings. A patient's BRCA1 result should be visible to their oncologist, primary care physician, and pharmacist without a manual request each time. Interoperable digital infrastructure is the foundation for preventive care at scale through genomic medicine.
The practical implication for hospital administrators is direct. EHR integration is not an IT project. It is a clinical strategy decision that determines whether your genomic program generates measurable patient outcomes or just generates data.
What are best practices for patient engagement and ethics in genomic programs?
Patient engagement in genomic screening is not a communication task. It is a clinical function that shapes whether patients act on their results. Pre-test counseling is the most critical phase for patient decision-making, and hospitals that treat it as a checkbox rather than a clinical encounter see lower rates of follow-through on recommended interventions.
The ethical and engagement framework for a well-run hospital genomic program includes these core elements:
- Informed consent that goes beyond a signature. Patients must understand what variants will be reported, what will not be reported, and what a result of uncertain significance means for their care. Genetic counselors, not administrative staff, should lead this conversation.
- Psychological preparation. A positive BRCA2 result or a Lynch syndrome finding carries significant emotional weight. Hospitals that offer psychological support resources alongside genetic counseling report higher patient satisfaction and better adherence to surveillance protocols.
- Clear communication of limitations. Genomic tests do not predict the future with certainty. Communicating probabilistic risk accurately, without either alarming or falsely reassuring patients, requires trained communicators.
- Privacy and data governance. Patients have a right to know how their genomic data is stored, who can access it, and whether it may be used for research. Transparent data governance policies are a prerequisite for building public trust in hospital genomic programs.
- Equity in access. Insurance coverage for genetic testing varies widely. Hospitals must build financial counseling into the pre-test workflow so that cost does not become a barrier to access for patients who would benefit most.
Hospitals that treat service design, digital maturity, and public engagement as core strategic priorities, rather than secondary concerns, build genomic programs that sustain adoption over time. The benefits of genetic counseling extend well beyond the test result itself. They shape how patients understand their health trajectory and whether they engage with the care plan that follows.
Key takeaways
Hospitals that integrate genomic data into structured clinical workflows, invest in AI-assisted interpretation, and prioritize pre-test counseling deliver the most measurable patient outcomes from genomic screening programs.
| Point | Details |
|---|---|
| Counseling drives outcomes | Pre-test counseling is the most critical phase; it determines whether patients act on genomic results. |
| EHR integration is non-negotiable | Genomic data must be searchable and structured in the EHR, not stored as static PDF reports. |
| AI addresses workforce gaps | AI-driven platforms extend the capacity of genetic counselors by automating variant classification. |
| Lab partnerships reduce costs | Partnering with certified genomic labs lowers capital costs while maintaining clinical control. |
| Ethics and trust are strategic assets | Transparent data governance and informed consent are prerequisites for sustainable program adoption. |
Genomic medicine in hospitals: what i've learned watching programs succeed and fail
I have watched hospital genomic programs launch with significant investment and stall within 18 months. The pattern is consistent. Leadership treats genomics as a technology procurement problem rather than a care delivery redesign. They buy the sequencer, hire one genetic counselor, and expect volume to follow. It does not.
The programs that work share one characteristic: they design the patient experience first and the technology second. They ask what happens after a patient receives a positive hereditary cancer result, and they build the counseling, referral, and surveillance infrastructure before they scale testing volume. That sequence matters more than the platform they choose.
The AI integration question is real, but it is often framed incorrectly. The question is not whether AI can interpret genomic data. It can, and it does so with increasing accuracy. The question is whether the AI output writes into the clinical record in a way that the treating physician can act on without additional manual steps. Most systems I have reviewed still fail that test.
Hospital administrators who want to build durable genomic programs should invest in three things before anything else: a genetic counselor with program design experience, an EHR integration specialist who understands HL7 FHIR standards, and a data governance policy that patients can actually read and understand. The sequencing technology is the least difficult part of this work.
— Tarek
How Genematrix supports hospital genomic screening programs
Hospitals building or expanding genomic screening programs need a partner with certified laboratory infrastructure, AI-driven interpretation, and a track record in clinical deployment. Genematrix is a Chicago-based, CLIA-certified biotechnology company that delivers hereditary cancer screening, pharmacogenomics, and precision medicine services to hospitals and health systems nationwide.

The GeneMatrixAI platform is trained on more than 500,000 genetic profiles and delivers structured genomic reports within 72 hours. Specialized modules including GeneCancer, GenePGx, and GeneMind address the full range of clinical genomic use cases hospitals encounter. Explore Genematrix's genetic research and lab certifications to assess how their technology fits your hospital's genomic program requirements.
FAQ
What is the role of hospitals in genomic screening?
Hospitals coordinate the full genomic screening pathway, from pre-test counseling and sample collection through laboratory sequencing, clinical interpretation, and EHR integration. Their role is to translate genetic data into clinical decisions that improve patient outcomes.
How do hospitals integrate genomic results into patient care?
Successful programs embed genomic findings as structured, searchable data directly into the electronic health record rather than storing them as isolated PDF reports. This allows genomic data to inform clinical decisions at every future care encounter.
What staffing does a hospital genomic program require?
A functional program requires genetic counselors, medical geneticists, laboratory scientists, and IT specialists with EHR integration experience. The key bottleneck is genetic counselor capacity, not sequencing hardware.
How does AI support genomic screening in hospitals?
AI platforms automate variant classification and flag clinically significant findings for human review. This extends the capacity of a small genetics workforce and reduces the time required to move from raw sequencing data to a clinical report.
What ethical obligations do hospitals have in genomic screening?
Hospitals must obtain meaningful informed consent, protect patient data under clear governance policies, and provide psychological support resources alongside genetic counseling. Building patient trust through transparent practices is a core requirement for sustainable program adoption.