TL;DR:
- Pharmacogenomic testing analyzes your DNA to inform pain medication choices based on how your body processes drugs. It is most useful when current treatments fail or cause side effects, especially for opioids like codeine and tramadol. However, PGx has limitations and is just one tool within comprehensive pain management strategies.
If you've cycled through pain medications that either stopped working, caused intolerable side effects, or simply never helped, you already know that standard prescribing often feels like guesswork. Pharmacogenomic (PGx) testing offers a different starting point: analyzing your DNA to understand how your body processes specific drugs, so your care team can make more informed choices before you swallow a single pill. This guide walks you through what PGx testing actually delivers for chronic pain patients, how to prepare, what happens at each step, and how to set realistic expectations when you review results with your provider.
Table of Contents
- What is PGx testing and why consider it for pain?
- What do you need before PGx testing? (Preparation and requirements)
- Step-by-step: How PGx testing works for pain medication
- Interpreting your results: What changes, what stays the same
- Pitfalls and what to expect: Common questions and troubleshooting
- Why PGx for pain is both promising and overhyped: the real story for patients
- Take the next step with personalized genetic insights
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| PGx offers guided choices | PGx testing helps tailor some pain medications to your genetic profile, especially for codeine and tramadol. |
| Evidence is still emerging | Insurer policies and scientific studies show mixed results, so routine use in pain management is not universal. |
| Work with your provider | PGx insights should be discussed with your healthcare team and considered as part of your whole medication plan. |
| Know the limitations | PGx can reduce trial and error but is not a replacement for careful monitoring and symptom tracking. |
What is PGx testing and why consider it for pain?
PGx testing analyzes specific genes to predict how your body metabolizes certain medications. Instead of waiting to find out whether a drug works or causes harm through weeks of painful trial and error, the goal is to use your genetic profile to inform prescribing from the start. For chronic pain patients, where medication regimens can become complex over months or years, that kind of upfront data is genuinely appealing.
The science behind this is real. DNA testing and medication outcomes are closely connected, particularly for drugs that rely on specific liver enzymes for activation or clearance. But it's equally important to be honest about the limits: as one major insurer's policy states, PGx testing for pain "is investigational and no FDA-approved genetic tests for pain management were identified." That doesn't mean the testing has no value. It means patients need to understand exactly where the evidence is strong and where it is still developing.
Here's a quick comparison of what PGx testing can and cannot reliably do for pain:
| What PGx can help with | What PGx cannot yet reliably predict |
|---|---|
| CYP2D6 metabolism status for codeine/tramadol | Whether a medication will fully relieve your pain |
| Identifying poor or ultra-rapid metabolizers | Your subjective pain tolerance or sensitivity |
| Flagging drug-gene interaction risks | Outcomes for most non-opioid pain drugs |
| Supporting personalized dosing conversations | Efficacy of physical or behavioral pain interventions |
The drug-gene interaction testing field is advancing quickly, and clinician adoption is growing, particularly for complex, multi-drug pain cases. Some advanced lab testing programs are already integrating PGx data into routine care. The most important takeaway for you as a patient is that PGx is a tool, not a transformation. Used well, it sharpens clinical decisions. Used with inflated expectations, it leads to frustration.
Key reality check: PGx testing is most useful when your current medication plan isn't working, when side effects are disruptive, or when you're starting a new drug regimen. It is not a substitute for comprehensive pain care.
What do you need before PGx testing? (Preparation and requirements)
Knowing what PGx is, you'll need a few key pieces in place to actually try it for your pain management plan. Not every chronic pain patient is the ideal candidate for PGx testing right now. The patients who tend to benefit most share a few common traits: they've tried multiple medications without adequate relief, they've experienced unexpected side effects, or their provider is considering adding opioids like codeine or tramadol to their regimen.
Research confirms that CYP2D6-guided approaches for opioid prodrugs are the most actionable, while evidence for other opioids remains heterogeneous. In practical terms, this means PGx is most decision-relevant when those specific prodrugs are on the table, not as a general-purpose solution for all pain medications.
Here's what you'll want to have ready before your appointment:
- A complete medication list, including all prescription drugs, supplements, and over-the-counter products
- A summary of your pain history, including which medications you've tried, what worked, and what caused problems
- Insurance information and prior authorization details, since most payers still classify pain-related PGx as investigational
- A willing prescriber, ideally one with experience interpreting pharmacogenomic reports
- Basic familiarity with terms like CYP2D6 and metabolizer status so you can have a productive conversation
Here are the patients least likely to benefit from PGx testing for pain right now:
- Those whose pain is well-controlled on current medications with no side-effect concerns
- Patients whose pain regimen involves drugs not significantly affected by known PGx markers
- Anyone expecting PGx to reveal a single "correct" medication that will resolve their pain
| Preparation step | Why it matters |
|---|---|
| Doctor consultation | Ensures clinical context for interpreting results |
| Full medication list | Reveals potential drug-gene interactions |
| Insurance check | Avoids unexpected out-of-pocket costs |
| Understanding key pharmacogenomic markers | Prepares you for meaningful results review |
| Realistic expectations | Prevents frustration with limited scope of results |
Pro Tip: Write down every single substance you take, including fish oil, melatonin, and any herbal supplements. Some of these can inhibit or induce the same liver enzymes your PGx test measures, which affects how your results are interpreted. This list could be the most important thing you bring to your appointment.
Step-by-step: How PGx testing works for pain medication
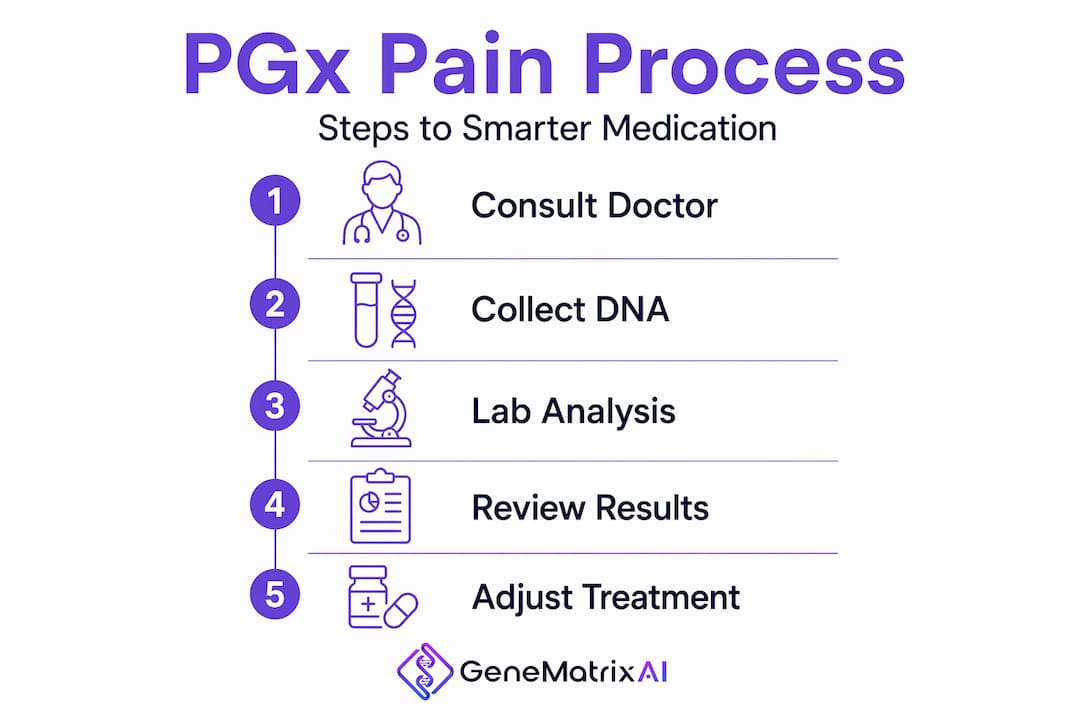
Once you're prepared, here's a step-by-step look at what PGx testing for pain actually involves. The process is more straightforward than most patients expect, and it doesn't require anything more invasive than a saliva swab in most cases.
- Consult your prescriber. Your provider reviews your pain history, current medications, and clinical goals to determine whether PGx testing is appropriate. They'll also handle ordering the panel.
- Order the PGx panel. A pharmacogenomic panel specific to pain and analgesic metabolism is ordered. This typically includes CYP2D6 at minimum, and often broader enzyme panels depending on your medication list.
- Provide your sample. Most panels use a simple saliva swab collected at home or in the clinic. Some labs use a blood draw. Either way, the collection is fast.
- Lab analysis. The laboratory sequences the relevant gene regions and identifies your specific variants. Turnaround time ranges from a few days to a couple of weeks.
- Report generation. A clinical report is generated that translates your genetic variants into a predicted metabolizer status and medication-specific recommendations.
- Provider reviews results with you. This is the critical step. Your prescriber (often alongside a clinical pharmacist) reviews your PGx report and discusses what adjustments, if any, are warranted.
The most important result for most pain patients is your CYP2D6 metabolizer status. This enzyme converts prodrugs like codeine and tramadol into their active forms. Your status falls into one of four categories:
- Poor metabolizer: Cannot activate codeine or tramadol effectively. These drugs are unlikely to work and carry specific risks.
- Intermediate metabolizer: Reduced conversion. Lower efficacy and altered risk profile.
- Extensive metabolizer (normal): Standard conversion. Typical drug response expected.
- Ultra-rapid metabolizer: Converts prodrugs too quickly. Risk of dangerously high active drug levels, particularly with codeine.
As research confirms, CYP2D6 polymorphisms directly impact exposure, efficacy, and safety for these specific drugs. Knowing your status before starting codeine or tramadol isn't optional in ideal clinical practice. It's the difference between a medication working as expected and a serious adverse event.
Pro Tip: At every pain management visit, bring up any medications that were added, stopped, or changed since your last appointment. Certain drugs can temporarily alter how your CYP2D6 enzyme functions, which means your actual drug response may not match your genetic prediction. Your provider needs this information to interpret your PGx results accurately.
Interpreting your results: What changes, what stays the same
With your PGx results in hand, here's how to interpret them for your pain treatment plan and what stays unchanged. The first thing to understand is the difference between your genotype (the DNA variants you carry) and your phenotype (how your body actually behaves with a given drug right now). These are not always the same thing.
A concept called phenoconversion is critical here. This occurs when medications you're already taking inhibit or induce the CYP2D6 enzyme, effectively changing your functional metabolizer status regardless of what your genes say. Research published in JAMA Network Open confirms that concomitant medications can alter PGx-based predictions in clinically significant ways. This is why your full medication list is so important, and why you should revisit your PGx interpretation whenever your regimen changes significantly.
Here's what your results report typically includes:
- Your CYP2D6 metabolizer status (and other relevant enzymes depending on your panel)
- Specific opioid recommendations or warnings tied to your status
- Notes on other genes that may affect non-opioid pain medications or co-prescribed drugs
- Potential drug-gene interaction flags based on your current medication list
What may change after PGx results:
| Clinical element | Likely to change? |
|---|---|
| Codeine or tramadol prescribing | Yes, if poor or ultra-rapid metabolizer status |
| Dose adjustments for affected drugs | Possibly, based on metabolizer status |
| Drug selection for new pain medications | Sometimes, with provider discretion |
| Guaranteed pain relief | No |
| Need for ongoing monitoring | No, PGx does not replace monitoring |
The clinical evidence on real-world outcomes is nuanced. CYP2D6-guided prescribing often changes medication choice but does not consistently improve pain outcomes in randomized controlled trials. A systematic review found reduced opioid use in some studies, but not reduced pain intensity. This is an honest, important finding, and one you should know before testing.
Safety note: Your PGx results may help refine your medication plan, but they do not replace medical advice, ongoing clinical monitoring, or the judgment of your prescriber. Never adjust medications based on genetic results alone.
Pitfalls and what to expect: Common questions and troubleshooting
Interpreting your results is just the start. You'll want to watch for some common pitfalls and set realistic expectations for what comes next. Many patients arrive at PGx testing hoping for a definitive answer, and leave feeling confused or let down because the results don't point to a single "right" medication.
Here are the most common mistakes patients make with PGx testing for pain:
- Expecting a magic bullet. PGx identifies genetic risks and guides some decisions. It does not diagnose your pain source or guarantee any medication will work.
- Not updating their medication list. If your medication regimen changes after testing, your results may need to be reinterpreted in light of new drug-gene interactions.
- Misunderstanding what genes the panel actually covers. Many panels focus heavily on CYP2D6 and a handful of related enzymes. Ask your provider exactly which genes were tested and which medications are covered by the results.
- Stopping medications without provider guidance. Even if results suggest a drug may be less effective for you genetically, stopping a medication abruptly can be harmful.
- Ignoring the insurance reality. As major payers have confirmed, PGx for pain is still classified as investigational by most insurers. Budget for potential out-of-pocket costs before ordering.
Pro Tip: Ask your provider to review your full medication list at every visit for new inhibitor or inducer interactions. Drugs like fluoxetine, bupropion, and several antifungal medications are strong CYP2D6 inhibitors. If any of these were added after your PGx test, your effective metabolizer status may be completely different from what your genetic report shows.
What to expect at your next one or two provider visits after testing: Your prescriber will likely review results in the context of your current regimen, potentially discontinue or adjust a prodrug, and may not make dramatic changes if your panel results are within normal ranges. The conversation itself has value. Think about genetic testing for prevention as a long-term strategy, not a one-time fix. For ongoing health management, the data you generate today informs decisions for years ahead.
Why PGx for pain is both promising and overhyped: the real story for patients
There's one more crucial perspective to keep in mind as you consider PGx testing for pain. We've seen hundreds of patients arrive expecting their genetic results to be a revelation. Sometimes they are. More often, they're one useful data point in a complicated clinical picture.
The honest truth: the clearest, most actionable use of PGx in pain management right now is identifying patients who should not be prescribed codeine or tramadol. Expert reviews confirm that CYP2D6 is the most actionable marker in pain pharmacogenomics, while other genetic markers remain insufficient for routine prescribing. That's a meaningful but narrow application.
What PGx does exceptionally well is change the conversation when standard medications fail or when side effects are disrupting a patient's quality of life. It gives prescribers a biological reason to pivot, rather than continuing to cycle through empiric options. That's genuinely valuable.
What it doesn't do is override the complexity of chronic pain itself. Pain is shaped by neurobiology, psychology, prior injury, sleep, inflammation, and social factors that no genetic panel touches. Patients who approach PGx as one layer in a broader, collaborative pain management plan tend to get more out of it than those who see it as the final word.
Bottom line for patients: PGx may meaningfully guide certain medication choices, particularly around codeine and tramadol. But it is not a universal solution for chronic pain. Your ongoing relationship with your care team, your willingness to document outcomes carefully, and your commitment to realistic expectations matter far more than any single test result.
Take the next step with personalized genetic insights
If you've been navigating chronic pain medications with limited guidance, understanding your genetic profile can change the quality of your conversations with your prescriber.

At Gene Matrix, our GenePGx module delivers CLIA-certified pharmacogenomic results through the GeneMatrix AI mobile app, designed to make your genetic insights accessible and actionable within 72 hours. Our AI platform, trained on more than 500,000 genetic profiles, interprets your results in the context of your full medication picture. Explore the Gene Matrix research and technology behind our testing standards, and review our affordable DNA testing plans to find the right fit for your ongoing health management needs. Personalized medicine starts with knowing your data.
Frequently asked questions
Does insurance cover PGx testing for pain?
Most insurers consider it investigational and do not routinely cover PGx testing for pain management, meaning many patients face out-of-pocket costs for this type of testing. Always verify your specific plan's coverage before ordering.
Which pain medications are most affected by PGx results?
Codeine and tramadol are the most impacted medications because they rely entirely on CYP2D6 metabolism to be converted into their active, pain-relieving forms. Poor or ultra-rapid metabolizers face meaningful efficacy and safety risks with these drugs.
Can PGx testing completely prevent side effects from pain medications?
No. PGx can flag genetic risk factors, but randomized controlled trials show no significant overall reduction in adverse events, though some studies found reduced opioid-related side effects in specific populations.
How often should PGx testing be repeated?
One test is generally sufficient since your DNA does not change, but phenoconversion from new medications can shift how your genes actually affect drug response. If your regimen changes significantly, your provider may need to reinterpret existing results in light of new drug interactions.