
TL;DR:
- Gene mutations are the main cause of cancer, with inherited mutations providing a significant risk window. Most cancers result from somatic mutations, but hereditary gene changes like BRCA1 and TP53 greatly increase individual risk. Genetic testing and counseling are essential for understanding and managing these risks effectively.
Gene mutations are the root cause of cancer, and understanding gene-cancer connections is the clearest path to knowing your real risk. Every cancer starts when DNA changes disrupt how cells grow, divide, or die. Some of those changes are inherited at birth. Most develop over a lifetime from environmental exposure, aging, or random copying errors. The distinction matters enormously, because inherited mutations like those in BRCA1, BRCA2, and TP53 can be detected before cancer appears, giving patients and families a genuine window for prevention.
Understanding gene-cancer connections: how mutations drive cancer
Cancer genes fall into two categories: tumor suppressor genes and oncogenes. Tumor suppressors, like TP53 and BRCA1, act as brakes on abnormal cell growth. Oncogenes, when mutated, act like a stuck accelerator. Cancer develops when these systems fail together.
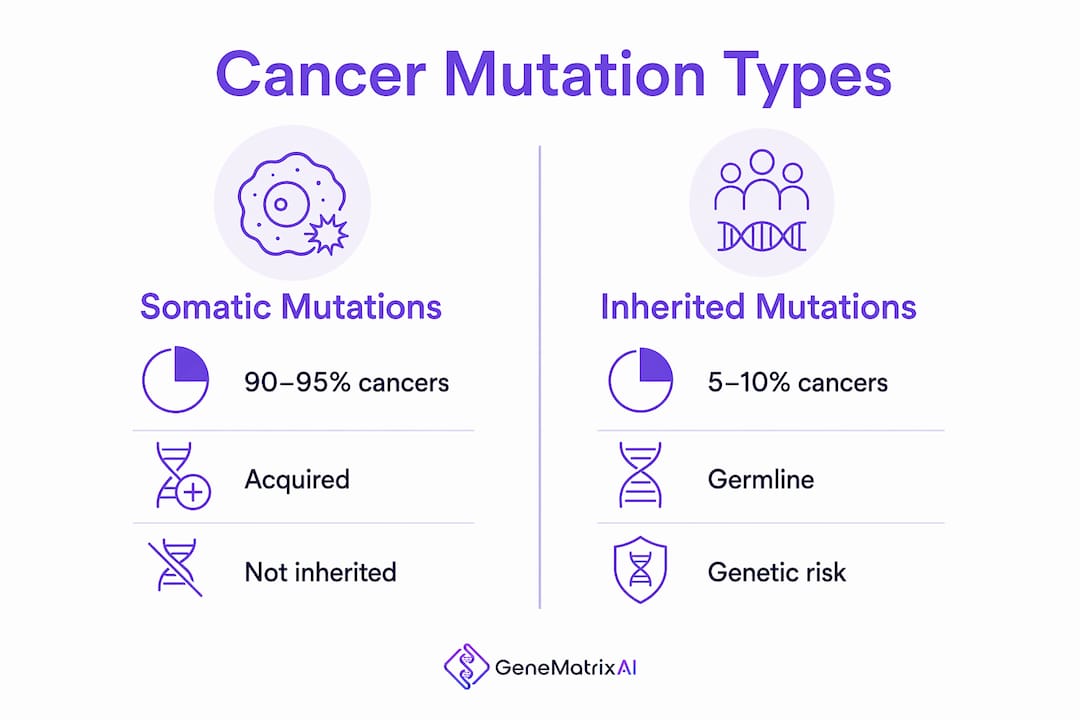
The distinction between germline and somatic mutations shapes everything about how cancer risk is inherited and managed.
- Germline mutations are present in every cell from conception. They are inherited from a parent and can be passed to children.
- Somatic mutations are acquired during a person's lifetime. They occur in a single cell and are not inherited.
- DNA repair genes like BRCA1 and BRCA2 normally catch and fix copying errors. When they malfunction, errors accumulate across cell generations.
- Tumor suppressor genes like TP53 stop damaged cells from dividing. A faulty TP53 lets abnormal cells multiply unchecked.
- Mutation accumulation is the key mechanism. Cancer rarely results from one mutation. It takes several failures in the same cell line.
Most cancers (90–95%) result from somatic mutations, not inherited ones. That means the majority of cancer cases are not written into a person's DNA at birth. Hereditary cancers are the minority, but they carry dramatically higher individual risk.
Pro Tip: Not every mutation causes cancer. Many mutations are silent or quickly corrected by the body's repair systems. Context, including which gene is affected and what other mutations are present, determines whether a mutation becomes dangerous.
Which inherited gene mutations carry the highest cancer risk?
Hereditary cancer syndromes are defined by specific germline mutations that substantially raise lifetime cancer risk. Three genes dominate the clinical picture: BRCA1, BRCA2, and TP53.
BRCA1 mutation carriers face a 65% lifetime risk of breast cancer and a 39% risk of ovarian cancer by age 70. Women without a significant family history carry a 9–12.5% breast cancer risk over the same period. That gap is not marginal. It represents a fundamentally different health trajectory that warrants active monitoring and, in many cases, preventive intervention.
Carriers of inherited TP53 mutations face a 90% chance of developing cancer by age 60. This condition, known as Li-Fraumeni syndrome, raises risk across multiple cancer types including breast cancer, brain tumors, sarcomas, and leukemia. It affects both men and women and can manifest in childhood.
The table below summarizes the most clinically significant hereditary cancer genes, the cancers they are linked to, and the approximate lifetime risk for carriers.
| Gene | Associated cancers | Approximate lifetime risk for carriers |
|---|---|---|
| BRCA1 | Breast, ovarian, pancreatic | Up to 65% breast, 39% ovarian |
| BRCA2 | Breast, ovarian, prostate, pancreatic | Elevated across multiple sites |
| TP53 | Breast, brain, sarcoma, leukemia | Up to 90% by age 60 |
| MLH1/MSH2 | Colorectal, endometrial (Lynch syndrome) | Substantially elevated |
BRCA1 carriers inherit one defective copy in every cell, which means every cell division carries a higher probability that the second copy will also fail. That second failure is often what triggers cancer. This two-hit model explains why inherited mutations are so much more dangerous than a single somatic event. Knowing your genetic risk assessment before symptoms appear is what makes hereditary cancer testing clinically meaningful.
How do co-mutations and gene interactions affect cancer progression?
Single gene mutations rarely tell the full story. Cancer progression depends on how multiple mutations interact across a tumor's genetic network. This is where recent cancer gene research has produced some of the most significant findings in oncology.
An AI-driven analysis of over 70,000 tumor samples across 119 cancer subtypes identified co-mutation patterns linked to metastasis and therapy resistance more reliably than any single gene analysis could. Co-mutations are combinations of mutations that appear together in tumors and collectively drive more aggressive cancer behavior. The finding reframes cancer from a single-gene problem to a network problem.
Key implications from this research include:
- Metastasis prediction: Certain co-mutation pairs predict whether a tumor will spread before clinical signs appear.
- Therapy resistance: Tumors with specific co-mutation profiles are more likely to resist standard treatments, including chemotherapy and targeted therapies.
- Tumor evolution: Cancer behaves like an evolving organism. Defective DNA repair creates genetic diversity within a tumor, and the most aggressive variants survive treatment.
- Precision oncology: Identifying co-mutation profiles allows oncologists to select combination therapies that target multiple vulnerabilities simultaneously.
AI and machine learning methods now classify mutations as gain-of-function, loss-of-function, or neomorphic, meaning they can predict how a specific mutation will change cell behavior. That classification directly informs which targeted therapy is most likely to work. Advances in cancer genomics research are making these predictions faster and more accurate every year.
Inherited single nucleotide variants affect genes governing DNA repair, energy production, and inflammation pathways, influencing cancer risk across multiple cancer types. Researchers have identified fewer than 400 key variants that shape these pathways. That number will grow as genomic databases expand, but it already points toward a future where inherited risk is mapped with far greater specificity than BRCA1 and BRCA2 alone.
What role does genetic testing and counseling play in managing cancer risk?
Genetic testing identifies whether a person carries mutations that significantly raise their cancer risk. The results can change screening schedules, inform preventive surgery decisions, and guide family members toward their own testing. But the process requires careful preparation and expert interpretation.
Genetic counseling is a prerequisite to testing, not an optional add-on. A genetic counselor helps patients understand what a positive, negative, or ambiguous result actually means for their health and their family. Without that context, test results can cause unnecessary anxiety or, worse, false reassurance.
Common outcomes from hereditary cancer testing include:
- Positive result: A known pathogenic mutation is identified. This triggers specific screening or prevention protocols.
- Negative result: No known mutation is found. Risk may still be elevated based on family history, so clinical follow-up remains important.
- Variant of Uncertain Significance (VUS): A genetic change is detected, but its clinical impact is not yet established. VUS results are common and require caution in interpretation, along with ongoing monitoring as research reclassifies variants over time.
The psychological weight of genetic testing is real. Learning you carry a BRCA1 mutation or a TP53 variant changes how you think about your body, your future, and your children's health. Counseling addresses that burden directly. It also helps patients communicate results to family members who may share the same inherited risk. Patients planning travel after a diagnosis may also want to understand their options for cancer-related travel coverage as part of broader life planning.
Pro Tip: Before your genetic testing appointment, write down three specific questions: What does a positive result mean for my screening schedule? What does a VUS result mean for my family? What follow-up is recommended regardless of the result? These three questions will make your counseling session far more productive.
A hereditary cancer testing guide can help you understand what to expect before you sit down with a clinician. Knowing the process reduces anxiety and helps you ask better questions.
Key Takeaways
Genetic mutations drive cancer by disrupting DNA repair and cell growth controls, and knowing which mutations you carry is the most direct path to managing your risk.
| Point | Details |
|---|---|
| Somatic mutations cause most cancers | 90–95% of cancers result from acquired mutations, not inherited ones. |
| BRCA1 and TP53 carry extreme risk | BRCA1 carriers face up to 65% breast cancer risk; TP53 carriers face 90% cancer risk by age 60. |
| Co-mutations drive aggressive tumors | Combinations of mutations predict metastasis and therapy resistance better than single genes. |
| VUS results require expert guidance | Variants of Uncertain Significance are common and need counseling and ongoing monitoring. |
| Genetic counseling is non-negotiable | Testing without counseling leads to misinterpretation and poor medical decisions. |
What I've learned from watching this field move faster than patients expect
The most common misconception I encounter is the belief that cancer is either "genetic" or "not genetic," as if those are two clean categories. They are not. Most people who develop cancer do not have an inherited mutation. Most people who carry a BRCA1 mutation do not develop cancer in their twenties. The gene-cancer relationship is probabilistic, not deterministic. That distinction is what makes genetic counseling so critical, and what makes oversimplified headlines so dangerous.
What has genuinely changed in the past few years is the scale of genomic analysis. Studying 70,000 tumor genomes simultaneously, with AI identifying co-mutation patterns that no human analyst could spot, is a different kind of science than sequencing one gene at a time. The findings are not just academically interesting. They are already shaping how oncologists choose combination therapies for patients with treatment-resistant tumors.
The part that still frustrates me is the gap between what research knows and what patients hear. A person can receive a VUS result, leave the clinic confused, and spend months in unnecessary anxiety because no one explained that "uncertain" does not mean "dangerous." That gap is a system failure, not a patient failure. Genetic counseling closes it. So does access to testing platforms that deliver results with clear, plain-language interpretation built in.
The most empowering thing a person can do right now is not wait for symptoms. Proactive genetic risk assessment, backed by proper counseling, gives you information you can actually use. That is what precision medicine is supposed to deliver.
— Tarek
Genematrix: hereditary cancer testing with clinical-grade precision
Genematrix is a CLIA-certified biotechnology company based in Chicago that delivers AI-powered hereditary cancer screening with results in 72 hours. The GeneMatrixAI platform is trained on 500,000+ genetic profiles and covers high-risk genes including BRCA1, BRCA2, TP53, and Lynch syndrome markers.

Every report includes plain-language interpretation and is designed to support informed conversations with your physician or genetic counselor. Genematrix's GeneCancer testing panel covers hereditary cancer risk assessment nationwide and worldwide. Patients who want to understand the science and certifications behind the platform can review the full research and lab standards that support every result. Proactive testing is not about fear. It is about having the information you need before you need it.
FAQ
What is the difference between inherited and somatic cancer mutations?
Inherited (germline) mutations are present in every cell from birth and can be passed to children. Somatic mutations develop during a person's lifetime in a single cell and are not hereditary. The vast majority of cancers result from somatic mutations.
How high is the cancer risk for BRCA1 mutation carriers?
Women with a BRCA1 mutation face a 65% lifetime risk of breast cancer and a 39% risk of ovarian cancer by age 70, compared to a 9–12.5% breast cancer risk for those without a significant family history.
What does a Variant of Uncertain Significance mean in genetic testing?
A VUS is a genetic change detected during testing that has not yet been classified as harmful or benign. It does not confirm cancer risk, but it requires ongoing monitoring and expert counseling as research continues to reclassify these variants.
Should I get genetic counseling before or after testing?
The American Cancer Society recommends genetic counseling both before and after testing. Pre-test counseling helps you understand what results mean. Post-test counseling helps you act on them appropriately, especially if results include a VUS or a positive finding.
Can AI improve how gene mutations are analyzed for cancer risk?
AI-driven analysis of large tumor datasets now classifies mutations by their functional effect, predicting whether they cause gain-of-function or loss-of-function changes. This directly informs targeted therapy selection and is making cancer gene research faster and more clinically useful.