
TL;DR:
- Next-generation sequencing is a fast, high-throughput technology that reads millions of DNA and RNA fragments simultaneously.
- It plays a central role in modern genomics, hereditary disease testing, and personalized medicine by enabling comprehensive genetic analysis.
Next-generation sequencing is defined as a massively parallel DNA and RNA sequencing technology that reads millions of genetic fragments simultaneously, delivering results in hours rather than months. The industry standard term is NGS, though you will also see it called high-throughput sequencing or next-gen DNA sequencing. Where Sanger sequencing processes one fragment at a time, NGS platforms from Illumina and Thermo Fisher Scientific can sequence billions of bases yearly in a single lab. That shift in scale is what makes NGS the backbone of modern genomics, hereditary cancer testing, and personalized medicine in 2026.
How does next-generation sequencing work?
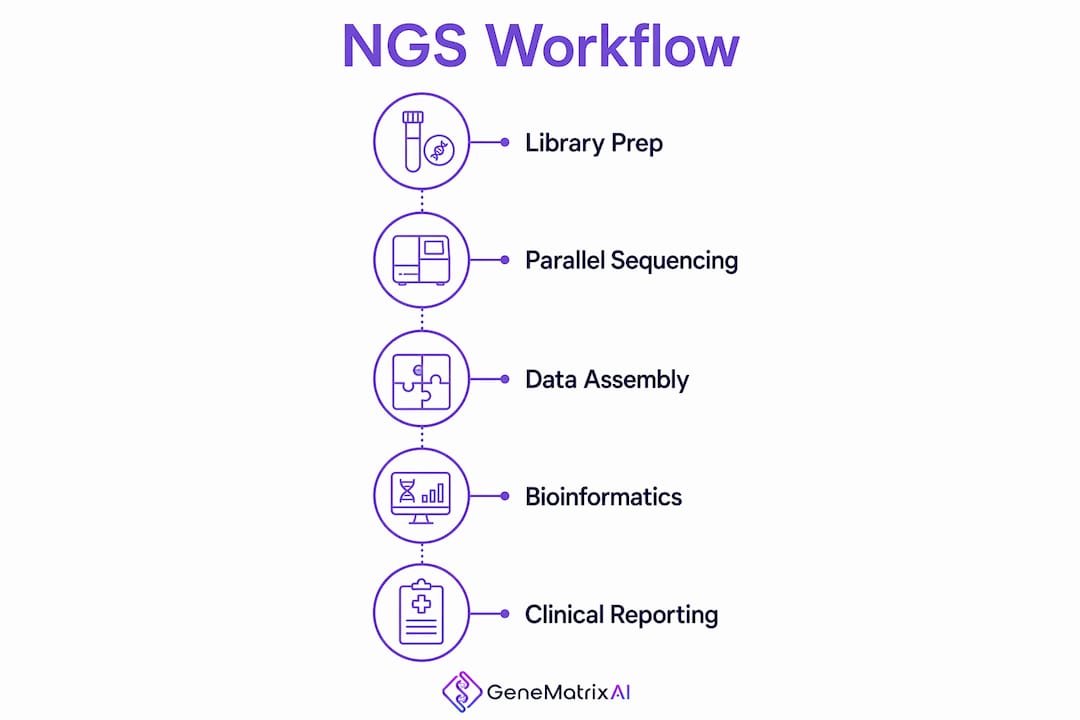
NGS converts a biological sample into a readable digital genome through four tightly linked stages. Understanding each stage helps clinicians and researchers interpret both the power and the limits of the data they receive.
1. Library preparation
Library preparation is the first and most consequential step. DNA or RNA is fragmented into short pieces, then short synthetic sequences called adapters are ligated to each fragment. These adapters allow the fragments to bind to a flow cell and serve as primers during sequencing. Poor library preparation produces biased or unusable data regardless of how powerful the sequencer is. This step is time-consuming, and labs that rush it pay the price in downstream analysis failures.
2. Massively parallel sequencing
Once the library is loaded onto a flow cell, millions of fragments are sequenced at the same time. This is the defining feature of NGS. Illumina's sequencing by synthesis method uses fluorescently labeled nucleotides. As each base is incorporated into a growing strand, a camera detects the emitted light signal and records the base identity. The process repeats across hundreds of millions of clusters simultaneously.
3. Data output and computational assembly
Raw signal data is converted into base calls, producing FASTQ files that contain billions of short sequence reads. Bioinformatics pipelines then align these reads to a reference genome, identify variants, and generate a report. Robust bioinformatics infrastructure is not optional. It is a core requirement that many clinical budgets underestimate at the planning stage.
Pro Tip: Before ordering an NGS panel for a patient, confirm that your lab or reporting partner has a validated bioinformatics pipeline specific to the gene panel you are using. Generic pipelines miss clinically relevant variants in targeted regions.
NGS vs Sanger sequencing: what are the key differences?
The comparison between NGS and Sanger sequencing is not about which method is better in absolute terms. It is about which method fits the clinical or research question.
| Feature | NGS | Sanger sequencing |
|---|---|---|
| Throughput | Millions of fragments simultaneously | One fragment at a time |
| Speed | Full genome in 24–48 hours | Days to weeks for large targets |
| Cost per base | Fractions of a cent (2026) | Significantly higher per base |
| Best use case | Whole genome, large panels, discovery | Targeted validation, single variants |
| Data complexity | High, requires bioinformatics | Low, direct readout |
The Human Genome Project cost nearly $3 billion and took over a decade. Modern NGS completes the same task for a few hundred dollars. That cost compression is the single biggest factor driving NGS adoption in clinical settings.
Sanger sequencing remains the gold standard for confirming specific variants identified by NGS, particularly in small-scale studies or when a single mutation needs clinical-grade validation. The two methods are complementary, not competing.
Key advantages of NGS over traditional methods include:
- Scale: NGS detects thousands of variants in a single run, where Sanger would require thousands of separate reactions.
- Sensitivity: NGS identifies low-frequency variants in heterogeneous samples, such as tumor biopsies with mixed cell populations.
- Flexibility: The same platform supports whole genome sequencing, targeted gene panels, RNA sequencing, and epigenomic analysis.
- Discovery power: NGS finds novel variants that no targeted Sanger assay would ever look for.
What are the main applications of NGS in healthcare?
NGS has moved from research tool to clinical standard across several medical specialties. The global impact of genetic testing reflects how affordable, accessible sequencing has reshaped what clinicians can offer patients.
Hereditary cancer risk assessment
Targeted NGS is the preferred method in clinical diagnostics for evaluating genes linked to hereditary disease risk. Panels covering BRCA1, BRCA2, and Lynch syndrome genes are now standard of care for patients with relevant family histories. Targeted panels offer higher sequencing depth than whole genome approaches, meaning fewer missed variants in the regions that matter most clinically.
Personalized medicine and pharmacogenomics
NGS data drives precision medicine decisions by matching patients to treatments based on their specific genetic profile. Pharmacogenomics panels identify variants in genes like CYP2D6 and CYP2C19 that predict how a patient metabolizes specific drugs. This prevents adverse drug reactions and guides dosing before a prescription is written.
Oncology and tumor profiling
Somatic NGS panels analyze tumor DNA to identify actionable mutations driving cancer growth. Genes like EGFR, KRAS, and ALK are routinely sequenced in lung cancer to determine eligibility for targeted therapies. Liquid biopsy approaches use NGS to detect circulating tumor DNA in blood, enabling non-invasive monitoring of treatment response.
Multi-omic research and population genomics
Multi-omic platforms combine NGS with transcriptomics and proteomics to build a more complete picture of disease biology. Population-scale biobanks like the UK Biobank and the NIH All of Us program rely on NGS to sequence hundreds of thousands of genomes, generating data that powers drug discovery and disease risk modeling.
Pro Tip: When selecting between a targeted panel and whole exome sequencing for a patient, consider the clinical question first. Targeted panels provide higher depth and faster turnaround for known hereditary conditions. Whole exome or genome sequencing is better suited for undiagnosed disease workups where the causal gene is unknown.
What challenges do clinicians face when using NGS?
NGS produces data at a scale that outpaces most clinical teams' ability to interpret it. The biggest challenge is not generating sequence data. It is determining what the data means for a specific patient.
Clinicians and researchers encounter four recurring obstacles:
- Variant interpretation: Many variants identified by NGS are classified as variants of uncertain significance (VUS). A VUS cannot guide clinical decisions without additional evidence, and its reclassification over time requires ongoing patient follow-up.
- Bioinformatics demands: Computational infrastructure for NGS data analysis requires specialized software, storage, and personnel. Hospitals that sequence in-house often underestimate this cost by a significant margin.
- Platform selection: Short-read sequencers dominate roughly 80% of the market but struggle with complex genomic regions, structural variants, and repetitive sequences. Long-read platforms from Pacific Biosciences and Oxford Nanopore resolve these regions but carry higher per-run costs.
- Test appropriateness: Clinicians are advised to carefully evaluate when NGS testing is warranted. Ordering a broad panel without a clear clinical indication increases the likelihood of incidental findings that create patient anxiety without guiding treatment.
Choosing the right clinical genomics provider reduces several of these burdens by shifting bioinformatics, variant curation, and report generation to a specialized team.
Key Takeaways
Next-generation sequencing is the most consequential technology in modern genomics because it makes comprehensive genetic analysis fast, affordable, and clinically applicable at scale.
| Point | Details |
|---|---|
| NGS is massively parallel | It sequences millions of fragments simultaneously, completing a human genome in 24–48 hours. |
| Library prep determines data quality | Poor fragmentation or adapter ligation produces biased results regardless of sequencing platform. |
| Sanger sequencing still has a role | It remains the standard for validating specific NGS-identified variants in clinical settings. |
| Interpretation is the hard part | Variant of uncertain significance classifications require ongoing curation and patient follow-up. |
| Platform choice matters | Short-read NGS suits most clinical panels; long-read platforms are needed for structural variants. |
Where NGS is actually headed, from where I sit
I have watched NGS move from a research curiosity to a clinical necessity in less than a decade. The technology itself is no longer the bottleneck. The bottleneck is everything around it: the bioinformatics, the variant databases, the clinical decision support, and the physician education.
What strikes me most is how many clinicians still treat NGS as a single test rather than a data-generating platform. A 50-gene hereditary cancer panel and a whole genome sequence are both "NGS," but they answer completely different questions and carry completely different interpretive burdens. Conflating them leads to poor test selection and disappointed patients.
The trend I find most significant is the move toward multi-omic integration. Combining NGS with transcriptomics and proteomics does not just add more data. It adds a different kind of data that explains why a variant causes disease in one patient and not another. AI-driven analysis platforms trained on large genetic profile datasets are beginning to make that integration clinically usable rather than just academically interesting.
My honest advice to any clinician considering NGS for their practice: start with the clinical question, not the technology. The test should follow the question. When you work with a reporting partner that delivers pre-interpreted, AI-curated results, the barrier drops considerably. The future of sequencing is not faster machines. It is smarter interpretation at the point of care.
— Tarek
How Genematrix uses NGS to deliver answers, not just data

Genematrix is a Chicago-based, CLIA-certified biotechnology company that applies NGS through its GeneMatrixAI platform, trained on over 500,000 genetic profiles. The platform delivers hereditary cancer genetic testing for BRCA1, BRCA2, Lynch syndrome, and dozens of additional hereditary risk genes, with reports returned within 72 hours. Genematrix also offers pharmacogenomics, psychiatric genetics, pediatric panels, and nutrigenomics under one platform. For hospitals, physicians, and health systems looking to move from reactive treatment to proactive precision medicine, you can explore the full scope of Genematrix's genetic testing science and certifications to understand what sets their approach apart.
FAQ
What is next-generation sequencing in simple terms?
Next-generation sequencing is a technology that reads millions of DNA or RNA fragments at the same time, allowing scientists and clinicians to analyze an entire genome in hours rather than years.
How is NGS different from Sanger sequencing?
NGS sequences millions of fragments simultaneously at a fraction of the cost, while Sanger sequencing reads one fragment at a time and is best used to confirm specific variants NGS has already identified.
What genes can NGS detect in hereditary cancer testing?
NGS panels routinely cover BRCA1, BRCA2, Lynch syndrome genes (MLH1, MSH2, MSH6, PMS2), and dozens of additional hereditary cancer risk genes in a single run.
Why does library preparation matter so much in NGS?
Library preparation determines whether the sequencer receives a representative, unbiased sample of the genome. Errors at this stage produce skewed data that no amount of computational analysis can correct.
What does a variant of uncertain significance mean in an NGS report?
A variant of uncertain significance (VUS) is a genetic change that has been detected but lacks sufficient evidence to classify it as disease-causing or benign. VUS classifications are reviewed over time as new data emerges.